Mother and son have received the same treatments on the same tooth - surprisingly! Both needed re-treatment. Dr. Danesh had to open up the calcified canals and fix so many complications. Two different generations, same tooth, same treatments & same challenging calcified canals.



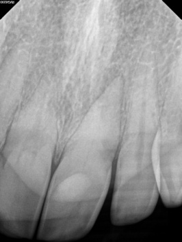
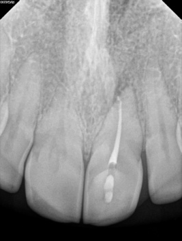
The distal apex was open to file # 100 due to an extensive resorption. It was ovoid-shaped as well, so it would never be sealed by a round gutta percha cone. MTA apical plug is recommended to achieve an adequate seal and a barrier to condense the filling material.



Treatment of a cervical resorption by internal approach.
Note the point of entrance was found and sealed with BC sealer and BC putty under microscope!

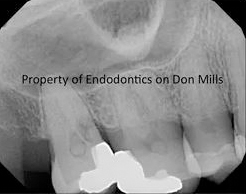
This patient was referred for tooth # 3.6 Re-t. Diagnosis was previous RCT and symptomatic apical periodontitis. Treatment options were offered and risks discussed.
She also was informed about the severe ledges in mesial canals and necessity of perio treatment before installing a crown.
She elected Retreatment. The ledges were negotiated to the apical foramen. The canals were filled with gutta percha and BC sealer. You may note osseous dysplasia at the periapical area! The follow up would be 1 year.
This patient was referred to Endodontics on Don Mills for tooth 3.6 re-treatment. The medical history was non-contributory. She reported recent flare-up, but once I examined her there were no symptoms. The patient was worried about fracture of the tooth rather than the extension of infection in the future. So, she sought for re-treatment.
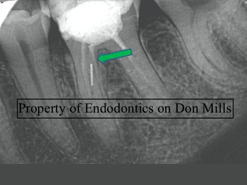

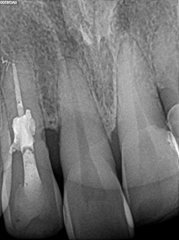
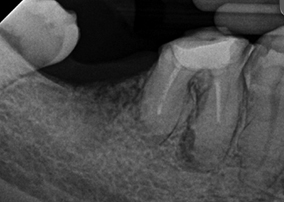
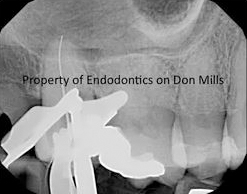
The available x-ray showed a large filling, previous RCT, broken instrument in one of the mesial canals, apical lesion and apical root resorption at the distal apex. The broken file could be in the middle mesial canal, as there was another path filled with the filling material (Picture 1). The diagnosis was previous RCT and asymptomatic apical periodontitis. Options like re-treatment, extraction, or no treatment was discussed with her. Also, pros and cons of each modality along with the risks were explained to her. In addition, she was informed of the risks associated with the broken instrument removal such as perforation, leaving the canal with thin walls, resistant file, etc. She opted for re-treatment, followed by a full coverage by her dentist. The prognosis of treatment was discussed.
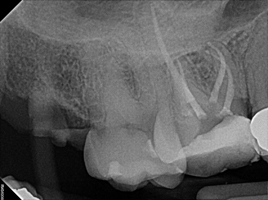
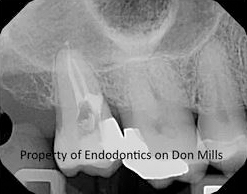
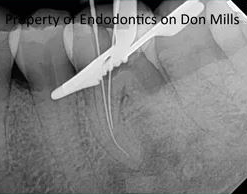
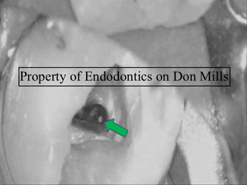
Having removed the coronal filling material and gutta percha from the canals, it turned out that the file has been broken in mesial-lingual (ML) canal, and the other path was an internal deviation from the original ML canal, most likely created in an attempt to remove the broken file or before the file breakage to find the ML canal. There was no middle mesial canal. Then, the coronal third of the ML canal was enlarged very gently with a thin ultrasonic (US) diamond coated tip. Next, the dentin around the coronal 2-3 mm of the broken file was removed with a very tinny non-diamond US tip (Picture 2). It gave me room to bypass the file and play around it to loosen it up. At the end, the same US tip was used in a contra-clockwise motion to disengage and remove the file.
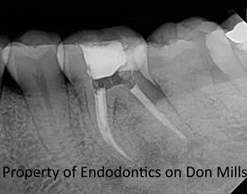
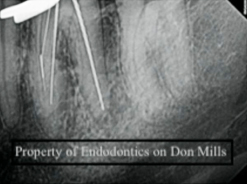
Finally, the canals received standard root canal treatment. The patient was referred to her dentist to restore the tooth and complete the coronal seal. She was booked after a year for follow up.